
Many news outlets this past week have produced reports questioning the need to floss. A report from The Associated Press (AP) claims to have looked at 25 studies on the subject and considers the data supporting flossing to be “weak.”1 Flossing was also left off the 2015-2020 U.S. Dietary Guidelines (a report published every 5 years by the Dietary Guidelines Advisory Committee, or DGAC). According to the American Dental Association (ADA), the omission of flossing from DGAC was a deliberate decision to focus on food and nutrient intake, with a focus on the effects of added sugar.2 Also cited by the AP is a 2015 study published from the Journal of Clinical Periodontology (gum and oral bone specialists) that reviewed the existing research on the subject of “interdental cleaners,” including floss, toothpicks, and oral irrigators, and found, “There is weak evidence in supporting the use of dental floss.”3
This puts dentists in an unusual position. Our principles and practices are supposed to be based in rigorous scientific research. So if something is not supported by hard science, then why are we recommending it?
There may be members of the general public that assume the recommendation of daily flossing is a scam just to sell floss. In response to that I would like to lay out the following points:
1. I make no money from floss or teaching patients how to use floss correctly. I give samples away at cleaning visits (that I pay a dental supply company for) and my hygienist and I spend time teaching our patients how to use it properly. Insurance companies do not pay us to do this – there is a code to bill for for oral hygiene instructions, but most dental insurance companies do not reimburse for it so we do it as a courtesy to the patient. There is no financial incentive to tell patients to floss. It is purely coming from a perspective of trying to help the patient avoid pain that results from some cavities and the loss of teeth that are beyond the point of being saved.
2. It would financially be better for dentists if no one flossed – ever. This would mean more gum disease, more cavities, more fillings, more root canals, more crowns, more implants, etc. In other words, less flossing results in more opportunities for work (and therefore more money) for dentists.
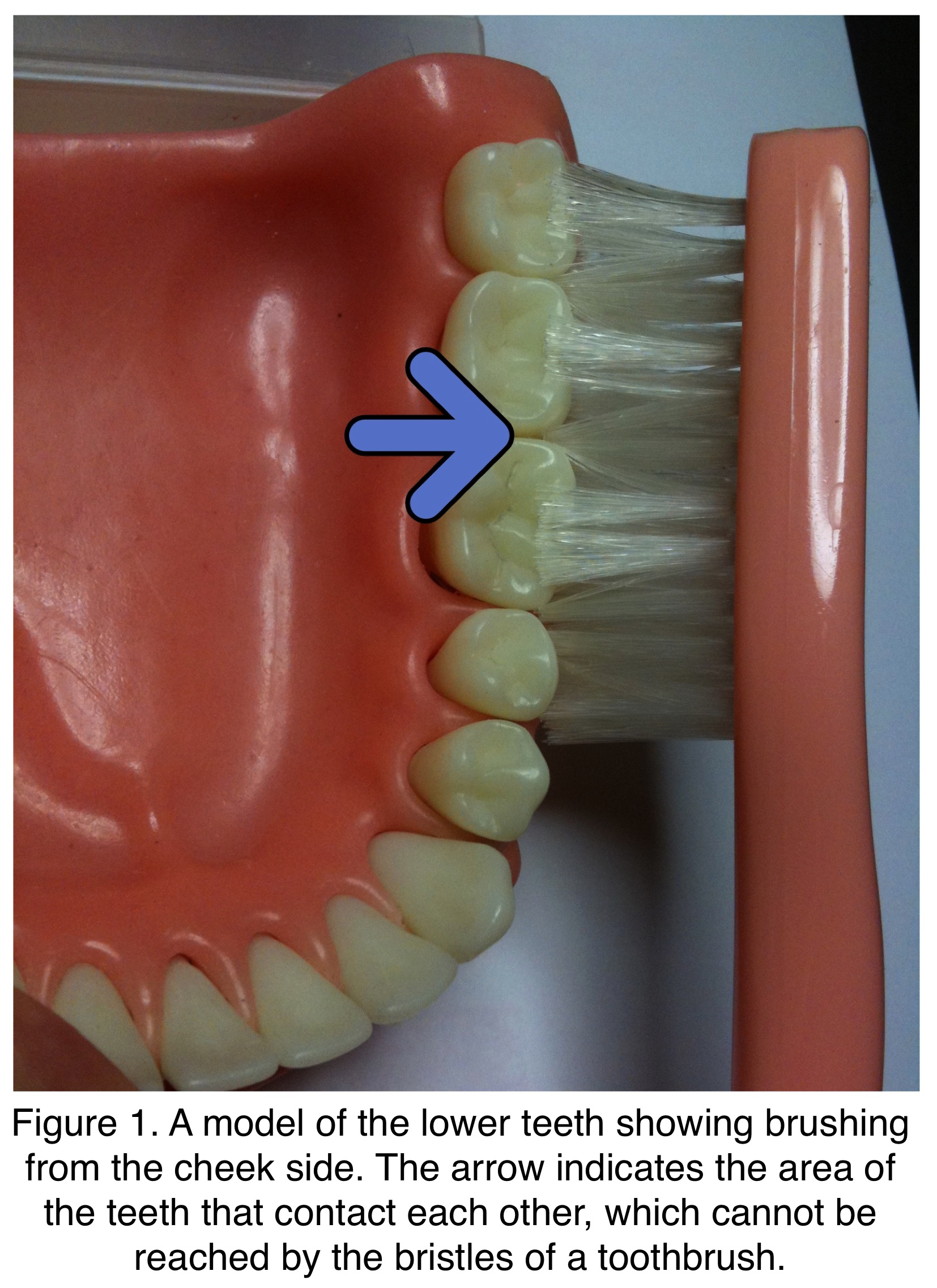
Since there is limited data supporting my second point, how can I be so sure that less flossing causes more dental problems? The surfaces of the teeth that make contact with other teeth are where food we eat mix with bacteria, form dental plaque, and this plaque then deposits on all surfaces of the teeth, especially along the gumline and in between the teeth. A toothbrush cannot reach all the way in between teeth and fully clean the surface of a tooth that is touching another tooth. (Figure 1)
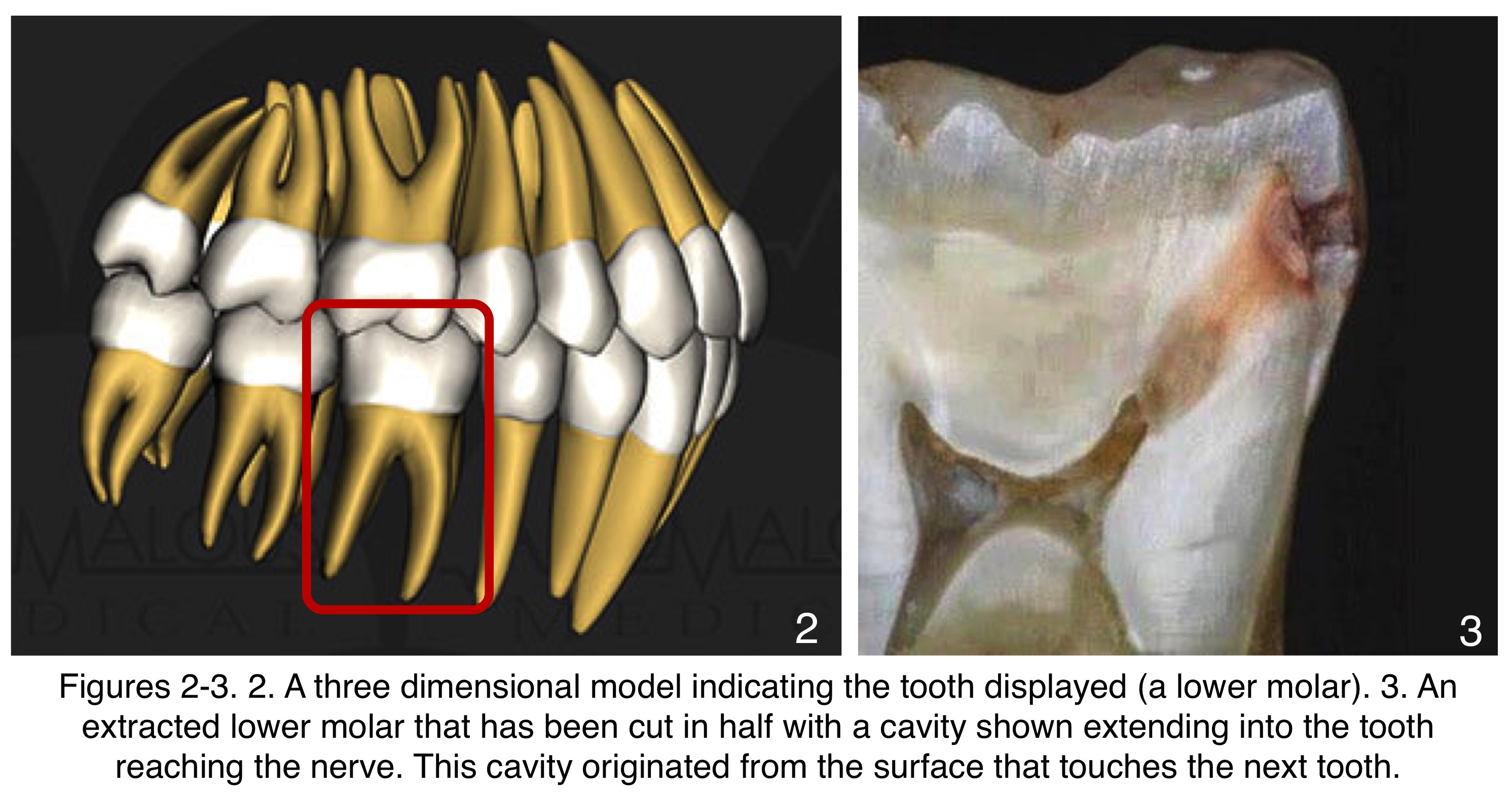
Over time, this plaque can cause rotting of the teeth as well as inflammation of the gums, which can cause not only tooth loss but may contribute to diseases that affect other systems of the body.4 Shown below is a tooth cut in half to show an in-between-the-teeth cavity that reached the nerve of the tooth. (Figures 2, 3)
Why is there a lack of evidence to support that flossing is important? My opinion is that an effective design of an experiment for this is very difficult for a number of reasons:
1. Design of an experiment that asks people not to floss for a long period of time and measures their oral health against people who do floss may be unethical. If the non-flossing group ends up with lots of cavities or lost teeth requiring a lot of time and money to repair, that would negatively affect the test subjects’ quality of life and long-term health.
2. Everyone’s mouth is different. Due to differences in not only diet and oral hygiene habits, but genetics and the types of oral bacteria present, people have different risk factors for both cavities and gum disease. Some people can go years without professional oral health care and have no issues. Others can be very prone to cavities and/or gum disease if they do not have good home care and get regular professional cleanings. Others still may have good home care and go to the dentist regularly but still have problems that require treatment. These differences in risk factors for dental problems can make a controlled study to measure flossing effectiveness difficult to standardize.
3. If a study is relying on the activities of someone outside of a laboratory setting (i.e., taking someone at their word to floss properly at the prescribed intervals), there may be some inaccuracies. All patients may not floss using proper technique or at every interval 100% of the time.
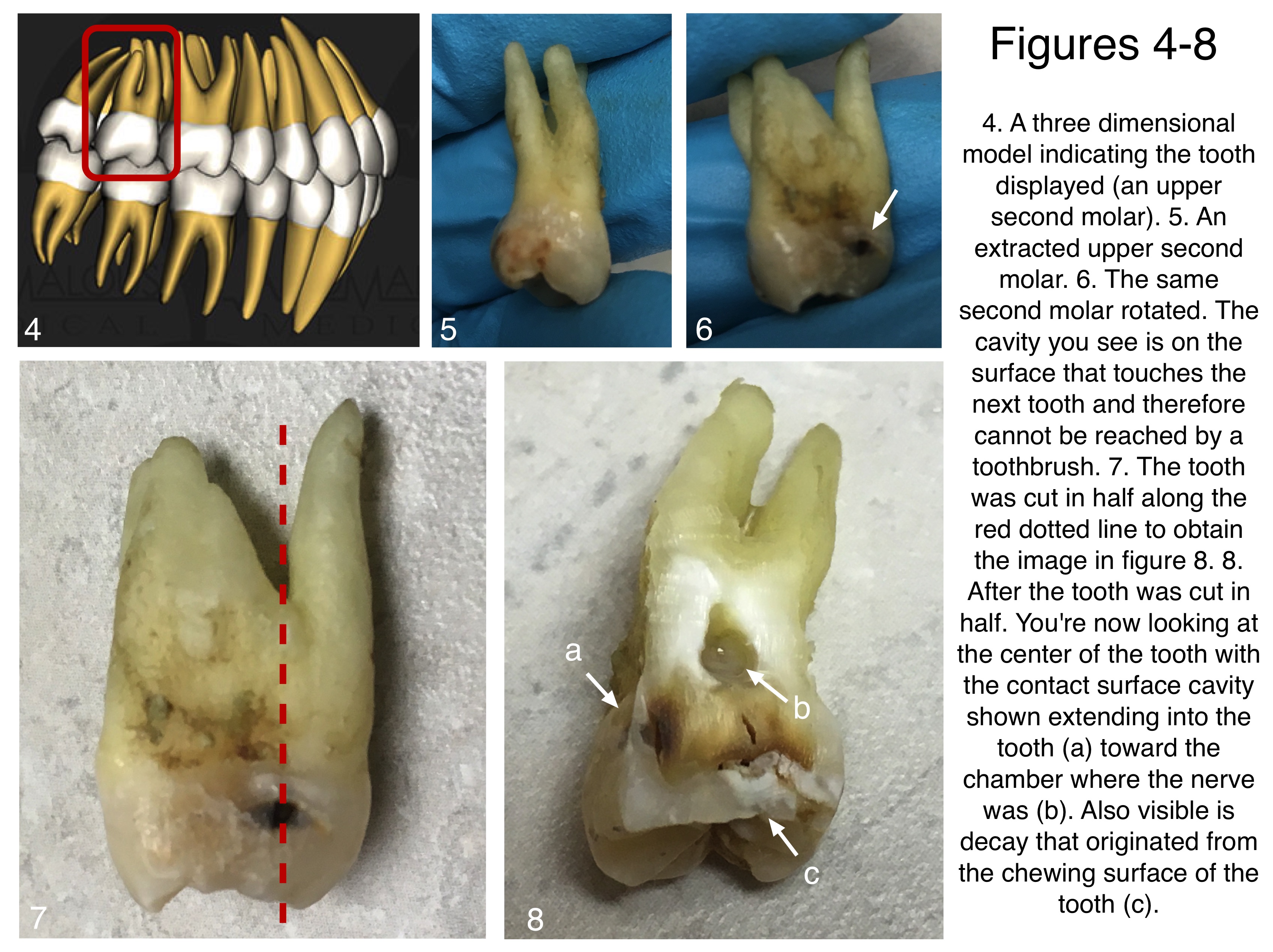
In search of my own hard evidence, I did some independent research. I took a tooth that I extracted and found a cavity on a surface that was touching another tooth (could not be reached by a toothbrush) and cut it in half. In this case you can see decay coming from both the side of the tooth and the chewing surface of the tooth. (Figures 4-8) As a dental professional I see cavities that originate in between teeth every day. Common sense tells me that flossing this area of the teeth regularly can only reduce the risk of cavities of this nature.
In conclusion, while the dental scientific community clearly needs to do a better job of proving the validity of flossing, it still makes all the sense in the world to me. My feelings on the matter come from my clinical training, my clinical experience, and common sense. I still talk to my patients about flossing, recommending it at least once a day. I floss at least once a day. There are other interdental tools that my patients like such as toothpicks, interdental brushes (such as GUM Proxabrush Go-Betweens®), or oral irrigators (such as Waterpik®), which can all be helpful. For patients with large spaces in between their teeth, the interdental brushes can be more effective than flossing alone in cleaning the area effectively. However, I still advise flossing as well to help fully clean the areas where teeth touch. Perhaps this recent media attention will motivate the dental research community to better prove the value of flossing.
Check out our Youtube Channel for educational videos about dentistry, our practice, and more!
References:
1. Donn, J. (2016, August 2). Medical benefits of dental floss unproven. Retrieved from https://www.washingtonpost.com/national/health-science/medical-benefits-of-dental-floss-unproven/2016/08/02/ea2e991a-5866-11e6-8b48-0cb344221131_story.html?tid=a_inl.
2. Federal Government, ADA Emphasize Importance of Flossing and Interdental Cleaners. (2016, August 4). Retrieved from http://www.ada.org/en/press-room/news-releases/2016-archive/august/statement-from-the-american-dental-association-about-interdental-cleaners?source=PromoSpots&medium=ADAHomeRotator&content=Flossing.
3. Sälzer S, Slot DE, Van der Weijden F, Dörfer CE. Efficacy of inter-dental mechanical plaque control in managing gingivitis – a meta-review. J Clin Periodontol. 2015 Mar; 42(S16):S92-S105. DOI 10.1111/jcpe.12363. Pubmed PMID 25581718.
4. Kuo LC, Polson AM, Kang T. Associations between periodontal diseases and systemic diseases: a review of the inter-relationships and interactions with diabetes, respiratory diseases, cardiovascular diseases and osteoporosis. Public Health. 2008 Apr;122(4):417-33. DOI: 10.1016/j.puhe.2007.07.004. Epub 2007 Oct 29. PubMed PMID 18028967.
Leave a Reply
You must be logged in to post a comment.